#BlackLives: Policies to reduce health vulnerabilities need better data quality
Experts point to the need for information that combines variables such as race, gender and age to overcome inequalities between blacks and whites in the area.
Sexually transmitted infections, maternal deaths: including deaths from septic abortions (when the fetus is not completely eliminated, causing infection), leprosy, tuberculosis, and Chagas' disease. These are some of the avoidable and more frequent health problems in the black population, both in comparison with the white contingent and in relation to national averages, in certain cases.
In addition to being more exposed to the risk of intentional violent death - as the Vidas Negras (Black Lives campaign) has warned -, blacks are also part of the group of Brazilians who have, in general, worse health indicators, expressed in the higher incidence of diseases and injuries with or without direct connection to each other. That's what official statistics reveal.
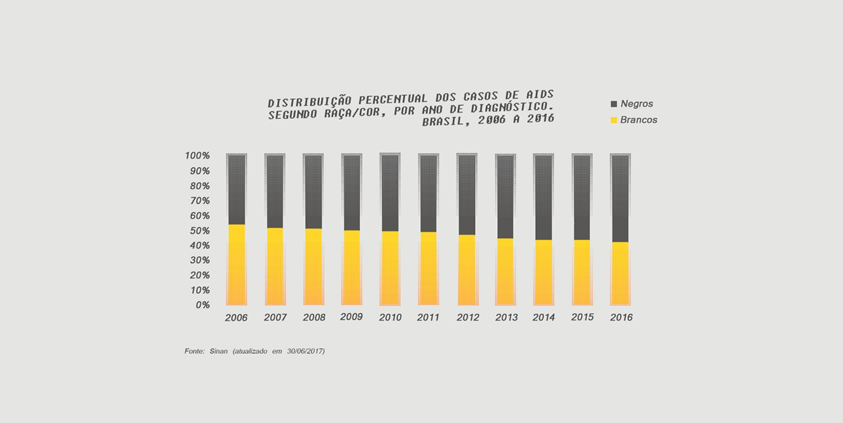
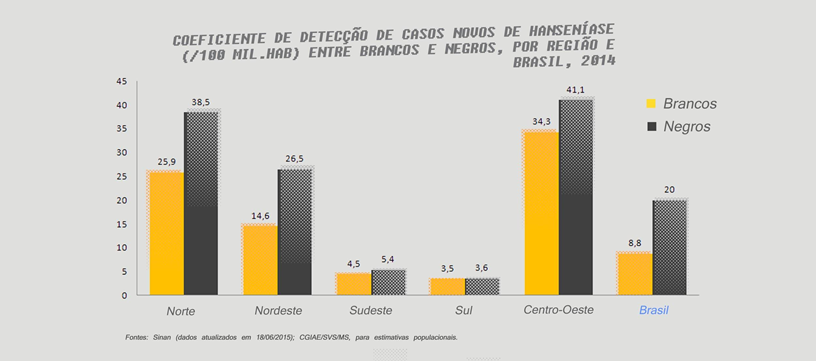
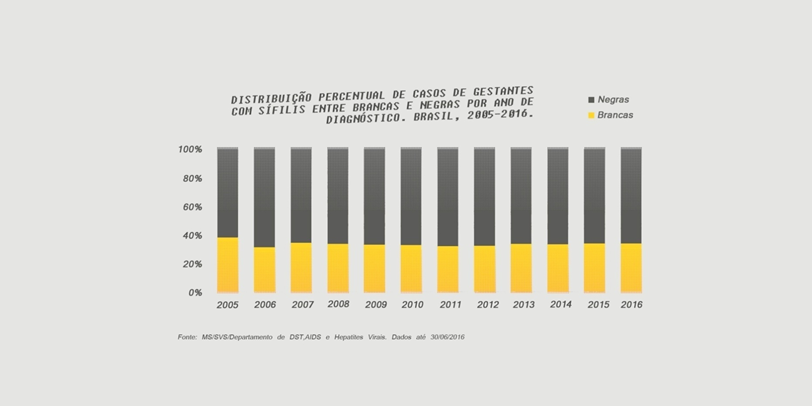
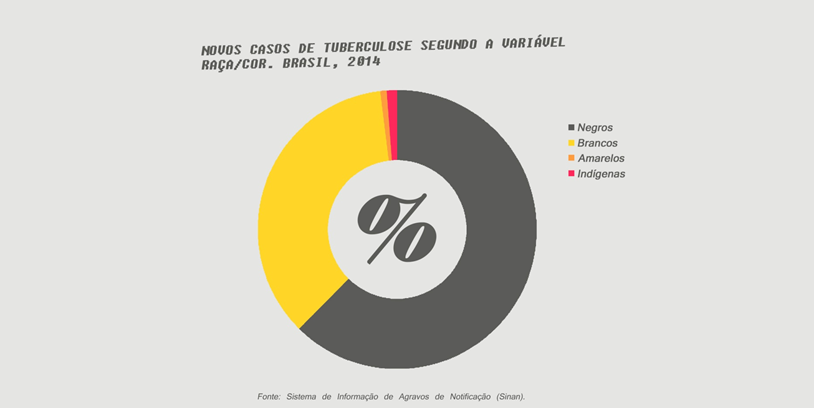
According to the Ministry of Health, 55% of registered cases of AIDS in 2016 occurred in black people and 43.9% in white people. Deaths from the disease also affect more blacks (58.7%) than whites (40.9%). In the same year, 38.5% of reports of acquired syphilis occurred among white people and 42.4% in black. Of the pregnant women diagnosed with syphilis, 59.8% were black and 30.6% white. Regarding the race/color of mothers of children with congenital syphilis, blacks were more than twice as much (65.1%) as white women (25.0%). Leprosy, an infectious disease caused by bacteria whose transmission is related to poor housing and hygiene, in 2014 had 31,064 reported cases, more than two-thirds (21,554) in the black population. In the tuberculosis registries, in the same year, 57.5% of the people who had the disease were black.
"The black population is not a sick population," says Lúcia Xavier, coordinator of the Criola black women's organization. "What happens is that they live with less quality." The group is more vulnerable to disease because it is under more influence from social determinants health, that is, the conditions in which a person lives and works, the unhealthy conditions, the low sanitary conditions to which he is subjected, and the sum of these various vulnerability indicators also increases the risk of losing his life, " she says .
According to the Ministry of Health, currently, 80% of the population that only has SUS as a health plan is black. According to the National Health Survey (2015), of the people who already felt discriminated in the services, by doctors or other health professionals, 13.6% highlight the racial bias of discrimination. The coordinator of Criola draws attention to the fact that unequal health performance has causes that go beyond possible restrictions or difficulties in accessing public services. "Studies show that racism is not a specific issue linked to the SUS and racism is also present in the private network", she says.
For Lucia, the confrontation with institutional racism must take place along with other measures to reduce racial inequalities. "The fight against institutional racism is fundamental to equity, but lack of health results from a number of other factors linked to racist practices." "How can a people who are discriminated against have a better quality of life?" she asks.
Poor data quality
The Pan American Health Organization (PAHO), following its recent Sanitary Conference of the Americas in September last year, recommended that Member States - including Brazil - promote public policies that address "ethnicity as a social determinant of health" . To this end, among other measures also suggested by PAHO, it is fundamental to: "have sufficient and quality data and generate evidence on ethnic inequities and inequities in health for political decision-making".
This is what Fernanda Lopes, an auxiliary representative of the United Nations Population Fund (UNFPA) in Brazil, pointed out. For her, the problem is precisely the non-adoption of the disaggregated data as a management tool. "In disaggregating data by race/color, inequities are evident, if these data are not used to guide policy, plans and programs, changes in living conditions and care do not happen. The indicators need to be sensitive: if they are not disaggregated, they will not be able to capture the real needs of the groups, there will be no right investments, inequalities will be maintained and/or aggravated", she says.
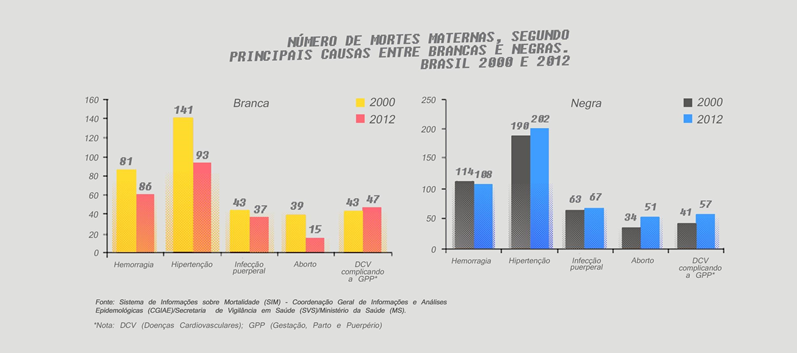
Vitória Lourenço, 25, surveyed the profile behind maternal deaths in Rio de Janeiro between 2009 and 2013, with information from the National Health System (DataSUS) database and data provided through the LAI Access to information). She found that mothers who die from pregnancy, childbirth, and postpartum causes in the state are young, black, and poorly educated. In Brazil, of all the maternal deaths of young people, the blacks are 55.3% while the white ones 47.5%.
Vitória, who is also a mother, drew attention to the issue of data quality, which has two main problems: the way information is processed and the fulfilment of the color question by health professionals. "There is still a taboo to ask how the person identifies himself and it is often at the discretion of the professional that he can enter 'white' to classify someone who identifies himself or herself. preferring to be identified as "black." In Rio, we do not have mandatory training for professionals about the importance of color, "she recalls.
Regarding the way data are processed, Vitória highlights a second problem, which is the low black presence in the production of research on race, racism and health. "We are usually just statistics, we are not in the spaces where we analyze data produced, and this has a direct impact on the knowledge we have about the subject." We are 53% of the population and because we do not know our reality? So many people? "
In the case of black youth, the issue of data quality is aggravated. Although there is disaggregated information on homicide and other external causes of death among 15-29-year-olds, data analysis explores, less than would be expected, combinations of race, gender, and age group. Gender identity, which is a risk factor for violent deaths in Brazil, does not even exist in health statistics.
For Fernanda Lopes, there is also a difficulty in speaking and working the health of the young population in a specific way, because traditionally one does not work health, but illnesses and diseases. "That state of physical, mental, and spiritual well-being described by the WHO as health can not be translated merely as an absence of signs and symptoms of illnesses, we know that health and disease are not works of chance or destiny. It is determined by economic, political, social, cultural, and environmental factors. Therefore, in order to achieve the state of well-being, diverse investments are necessary inside and outside the health service. If racism is not recognized and faced, black youth will not have health and will always be at greater risk of illness and death", she points out.
The importance given to the angle of illness has led to a cycle involving data production on one side and a look at the policies of another, both much more focused on external causes. This has generated a grey zone in relation, for example, to the knowledge of the more general health conditions of black youth.
"We do not know what affects this population beyond the external causes of death. We know the data on pregnancy, but we do not have anything about cancer, we know something about HIV/AIDS, but we do not know how prevalent sickle-cell anaemia is. We do not know about the quality of health care for young people, "says Lúcia Xavier.
Among the recommendations of the Sanitary Conference of the Americas is that data and information disaggregated make up the ethnic focus in the application of health strategies and action plans, according to the national realities. In Brazil, much about the living conditions and health of black youth is yet to be known. This is one of the fundamental steps to reach the goals of the Sustainable Development Agenda 2030 without any young people being left behind.
We thank our UN Online Volunteer, Juliana Nogueira, for her contribution to the translation of this article. Juliana is an online volunteer mobilised through www.onlinevolunteering.org.